An eight-practitioner physiotherapy clinic in Melbourne sees around 300 patients a week. If each 50-minute consult generates 15 minutes of notes, treatment plans, and outcome reporting, that is 75 hours a week of documentation overhead. Spread across a year, that is close to 1,400 billable hours gone to administration.
That is $210,000 of recoverable revenue at $150 per appointment hour. Most clinics do not frame it that way. They call it the job. That framing is expensive.
What the workflow actually does
Allied health documentation follows a predictable shape. The practitioner sees the patient, forms a clinical view, and then translates that view into written artefacts: SOAP notes, treatment plans, NDIS progress reports, outcome measure summaries. Claude handles the translation. The practitioner supplies the clinical view and approves the output.
The four workstreams that typically move to Claude in an allied health documentation deployment:
Notes drafting. The practitioner completes a structured consultation prompt covering diagnosis, presenting issue, and session observations. Claude generates a SOAP note draft. Typical time to review and save: under 3 minutes.
Treatment plan generation. Linked to the diagnosis and patient goals, Claude drafts a plan with relevant clinical guideline references where applicable. The practitioner adjusts for the patient's specific context.
NDIS progress reporting. The NDIA's narrative requirements are specific and time-consuming to draft from scratch. Claude generates a compliant draft against the participant's plan goals. Typically 5 to 10 minutes of practitioner review, not 45.
Outcome measure summaries. Pulled from the practice management system, Claude summarises progress against validated scales such as PSFS, SF-36, and DASS-21 for review notes and insurance reporting.
A Sydney occupational therapy clinic running this pattern recovered around 9 billable hours per practitioner per week. At a fully loaded practitioner rate of $120 per hour, that is roughly $56,000 per practitioner per year in freed capacity. The figures vary by clinic size, but they tend to be material. Run your own numbers through the ROI Calculator before deciding on scope.
The compliance frame
Allied health documentation in Australia operates under several overlapping obligations. AHPRA registration standards require contemporaneous and accurate record-keeping for physiotherapists, occupational therapists, speech pathologists, and psychologists. NDIS provider obligations add a second layer: progress notes must demonstrate functional progress against participant plan goals in a specific narrative format.
None of these obligations are incompatible with Claude-assisted documentation. The obligation is on what the record says and who reviews and attests to it, not on which tool produced the first draft.
The deployment pattern that meets these standards: Claude runs inside the clinic's accredited environment, patient data does not transit external APIs in identifiable form, and the practitioner reviews every output before it saves to the practice management system. What saves to the record is the practitioner's record. Our AI Automation Services include the technical architecture and compliance documentation for each deployment.
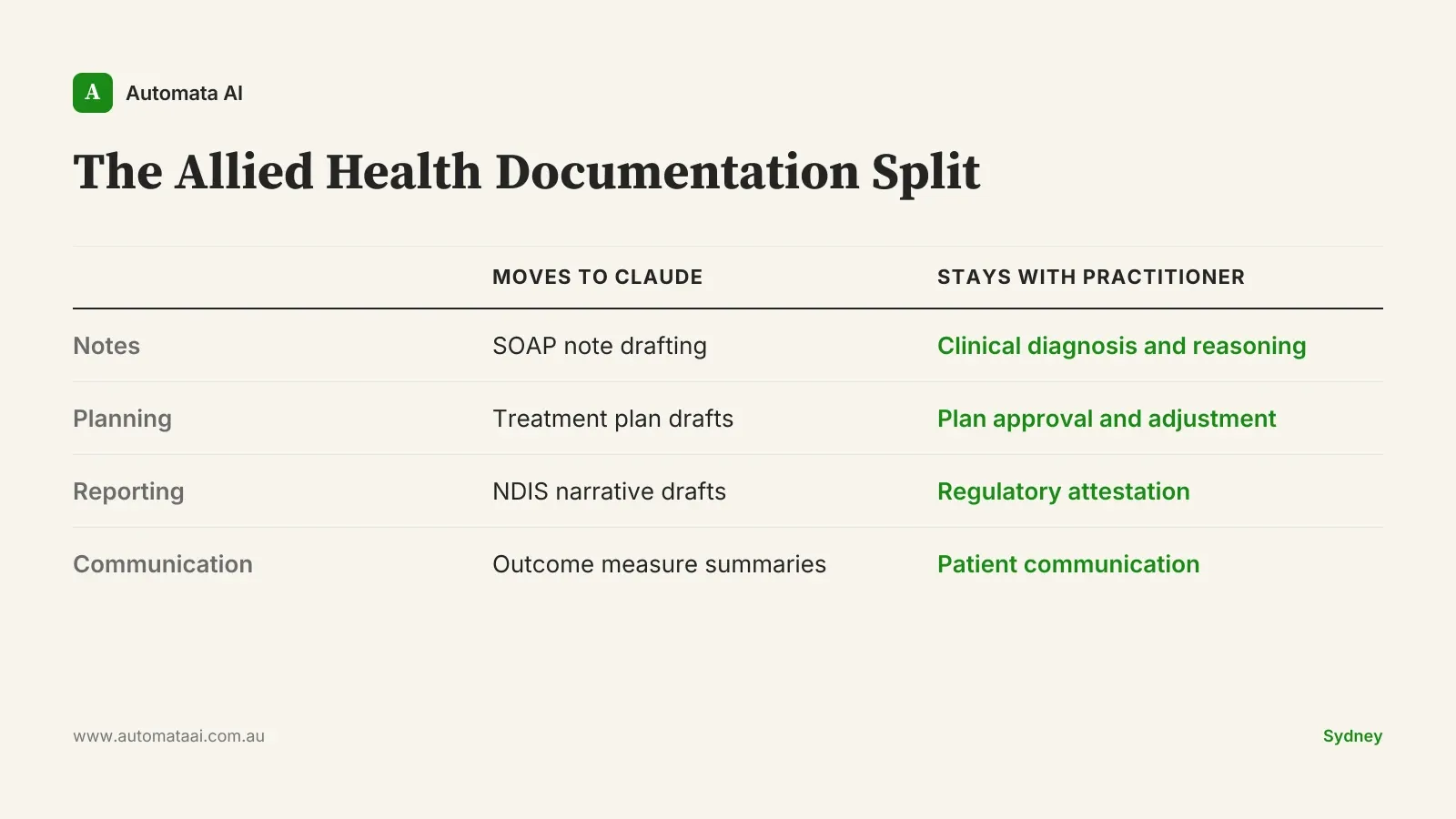
What stays human, what moves to Claude
The clinical decision is not negotiable. Claude does not diagnose, does not recommend treatment changes, and does not communicate with patients. Those stay with the registered practitioner.
What moves to Claude is the translation work: converting clinical observations into written form, formatting against the relevant standard, and cross-referencing prior session records for outcome summary purposes. The clinical reasoning stays human. The clerical labour does not have to.
The Allied Health Documentation Split is the framework we use when scoping these deployments. It draws a clear line between what the tool drafts and what the practitioner owns. Every Claude output carries a reference back to the session data it drew on. Practitioner review time averages under 3 minutes per artefact when the structured consultation prompt is completed.
When this is the wrong call
Not every allied health documentation problem is a Claude problem.
If practitioners do not have a consistent consultation structure — if notes vary because the clinical process varies — documentation tooling will not fix it. The tool has nothing structured to draft from. Get the consultation process stable first.
If the clinic has fewer than three practitioners, the economics change. At $150 per appointment hour, fewer than 450 billable hours are affected per year. The payback period stretches past 12 months. Not impossible, but the deployment usually needs a second justification: NDIS reporting quality, audit preparedness, or staff retention.
If the practice management system does not expose structured data, or patient records span both paper and digital, the integration scope increases materially before the documentation workflow can run. That is a data infrastructure problem. Solve it before scoping the documentation layer.
The rollout sequence that works
Australian providers that big-bang a new documentation workflow report adoption below 25 percent. The clinical team does not trust it, or edge cases emerge in week one and nobody knows what to do. Providers that roll out sequentially over six months hit adoption above 70 percent.
The reason is straightforward once you have seen both patterns. Practitioners need to build trust in the draft quality before they will reduce their review time. You cannot mandate that trust. You earn it by showing the numbers week over week.
Months 1 to 3. Notes only. One structured consultation prompt per clinical area. Measure draft quality and edit volume weekly.
Months 4 to 6. Expand to treatment plans. The practitioner approval step is non-negotiable.
Month 7 onwards. NDIS reporting. The highest-value workflow and the most sensitive. It goes last for a reason.
Automata AI builds allied health documentation workflows for Australian clinics. If you are mapping the documentation overhead and want to know whether the economics justify a deployment, the AI Readiness Assessment is the right starting point.
There is a second cost that does not appear in billable hours. When documentation overhead is the dominant part of a clinician's day, the work feels crushing. The practitioners spending 20 hours a week on NDIS reports are 20 hours away from the work they trained for. Clinics that deploy Claude-assisted documentation well report a measurable reduction in staff turnover in the first year — worth roughly $90,000 annually in reduced recruitment and onboarding for an eight-practitioner team.
That benefit is hard to model before rollout. It shows up in month nine or ten, when the team that was talking about leaving is not talking about it anymore.