A GP sees 35 patients a day in a busy suburban Sydney practice. The consults end at 6. The letters, billing queries, and compliance forms run until 8. That's not an unusual story. It's the baseline.
Most healthcare ROI conversations start from sector-wide numbers. That's the wrong shape for a board-level business case. A partnership at a 6-GP practice in Parramatta doesn't want to know what AI saves the NHS. They want to know what it saves them, in AUD, against a figure they recognise from their own P&L.
The hours that are actually recoverable
Letter drafting. Around 11 hours per GP per week in general practice, 8 hours per practitioner in allied health.
Billing and Medicare claims. Around 4 hours per practitioner per week in private practice.
Patient communication. Around 3 hours per practitioner per week.
Compliance documentation. Highly variable. Between 6 and 14 hours per practice per week depending on accreditation cycles.
A 6-GP general practice in suburban Sydney runs at roughly 132 hours of administrative overhead per week. That's approximately 6,800 hours a year. At a fully loaded GP cost of $340 per hour, covering salary, super, indemnity, and overhead, that puts around $2.3 million of clinical capacity into work that doesn't require clinical judgment.
The number is confronting. That's the point. Most practices have never added it up.
What a Claude rollout actually recovers
A realistic recovery rate sits at 50 to 70 percent of administrative hours. Some of that returns as clinical work: longer consultations, more patients, or both. Some returns as shorter days for practitioners who are already stretched. At 60 percent recovery, the 6-GP practice above frees roughly $1.4 million of latent capacity per year.
Not all of that becomes revenue. The realistic revenue-capture rate in our modelling is 40 to 60 percent, depending on whether the practice has demand headroom, meaning spare appointment capacity that can be filled. At 50 percent capture, the recovered revenue is around $700,000 a year. That's before accounting for the retention and recruitment effects that follow when GPs stop finishing consult sessions with two hours of letter-writing still ahead of them.

The cost frame
A privacy-first Claude rollout for a 6-GP practice runs approximately $180,000 in year one. That covers implementation, integration with practice management software, staff training, and data governance setup under the Australian Privacy Act. Ongoing costs sit at around $90,000 a year in steady state, covering model usage, maintenance, and support.
The break-even on recovered clinical revenue alone is around 7 weeks of captured capacity. At that payback period, the spreadsheet almost completes itself. The harder internal conversation is year one cash flow, not year three ROI. Running the numbers for your own practice takes about three minutes in our ROI Calculator.
When this model doesn't hold
There are three scenarios where the business case changes shape significantly.
Volume is too low. Solo practices and small two-GP partnerships don't generate enough administrative throughput to justify implementation at these numbers. The break-even shifts from 7 weeks to 18 months or longer when the practice has two GPs rather than six.
No demand headroom exists. If every GP's appointment book is full and the practice won't expand patient numbers, recovered time returns as shorter days rather than additional revenue. That's a quality-of-life improvement, but the revenue case needs to be framed differently to the board.
Rollout discipline is missing. Practices that measure no baseline before go-live, skip staff training, or attempt a simultaneous multi-site rollout consistently see 30 to 50 percent lower recovery than phased pilots. The model above assumes a phased rollout. Adjust it if yours isn't.
Three objections every healthcare board raises
The objections are predictable. That makes them easy to prepare for, and costly to ignore.
"Will patients accept this?" Patients interact with the GP, not the documentation system. Recovered time translates to longer consultations or reduced GP fatigue. Both improve the patient experience. The concern is manageable; it just needs to be addressed before the board meeting, not at it.
"What about Medicare audit risk?" The audit position is stronger with Claude than without it. Every action has provenance: date, time, model version, GP review and sign-off. Manual notes rarely carry that trail. Documentation quality improves.
"Will my staff resist it?" Practices that pilot properly see staff become the strongest advocates. Receptionists and practice nurses spend the most time on the categories Claude handles. Resistance typically lands with whoever wasn't included in the pilot design, not with the people who used it.
How to defend the case to a sceptical board
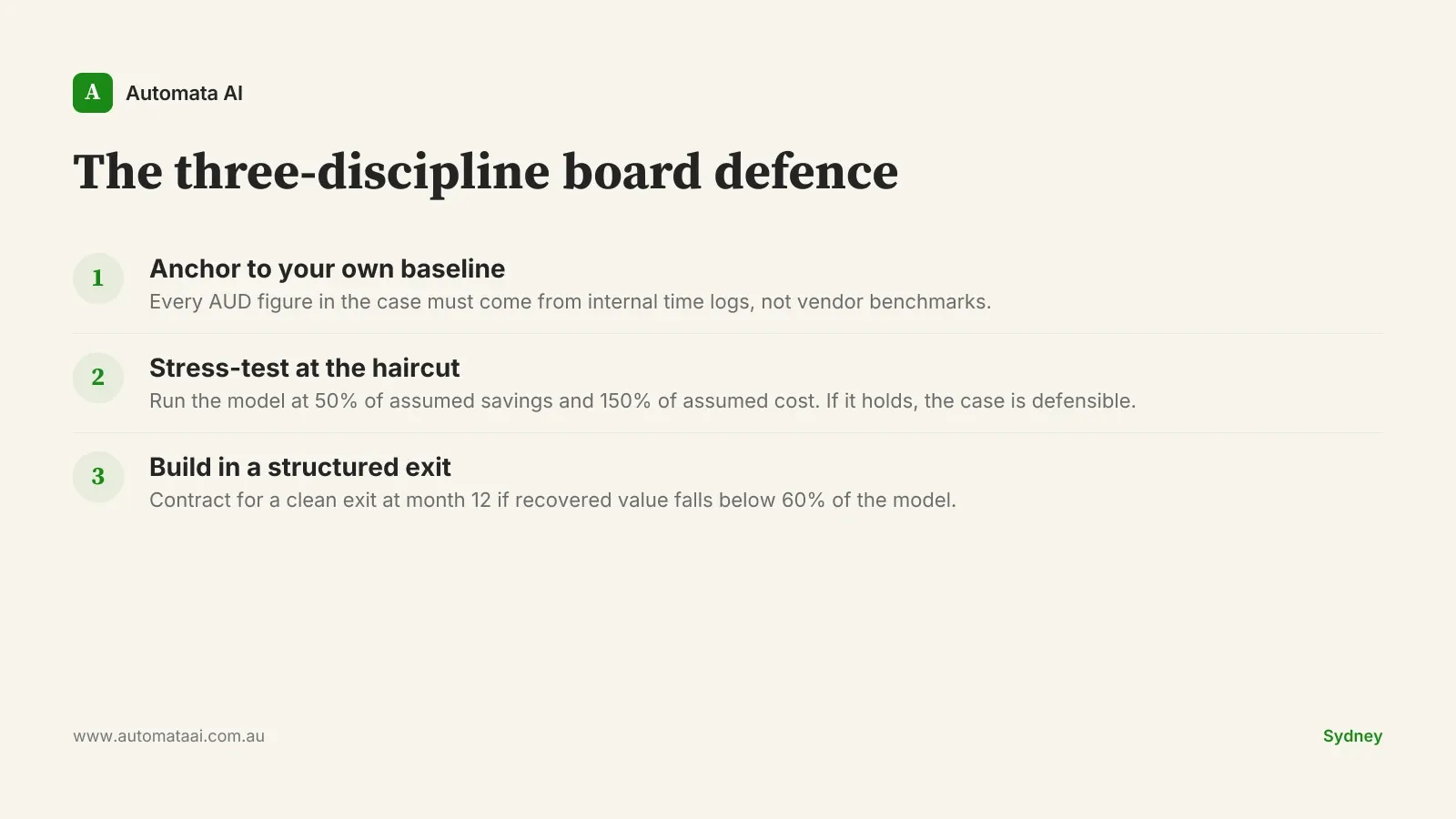
Boards that have watched vendor presentations for a decade discount productivity claims by default. The approach that works is to anchor every number to a measured baseline from the practice's own operations. A claim sourced from internal time logs survives scrutiny. The same claim sourced from a vendor document does not. Baseline measurement before go-live is not optional. It is the difference between a defensible business case and a brochure.
Sensitivity analysis is the second discipline. Run the model at 50 percent of the assumed savings and 150 percent of the assumed cost. If the case holds at that haircut, the board has a position they can defend publicly. If it doesn't hold, the case needs strengthening before it goes to the table.
The third discipline is a structured exit clause. The contract should permit a clean exit at month 12 if recovered value is below 60 percent of the model. Australian boards respond well to optionality framed in writing. A board that knows the downside is bounded approves faster than one that suspects open-ended commitment. The clause is rarely invoked. It matters anyway.
The AI Readiness Assessment we run with Australian healthcare practices is built around this pattern: measurable baselines, phased rollout, and a clear exit at month 12 if the numbers don't hold.
Pick one process. Measure the baseline this week. Model the payback at 50 percent of what you expect. If it still works, the case almost presents itself.