It is 7:15pm and the GP is still at her desk. Not seeing patients — writing. A referral to the cardiologist. An allied health summary for the physio. A WorkCover certificate that needs to match the consultation note from this morning. The clinical work finished an hour ago.
This is the hidden load in Australian general practice: letters. Claude can compress the drafting cycle. But only if the privacy architecture is built before the first workflow goes live.
The cost in plain numbers
A typical six-GP practice spends around 11 hours per week on letter drafting and correspondence. At a fully loaded GP rate of $340 per hour, that is roughly $190,000 a year in consulting time that never reaches a patient. A Claude workflow that handles 70 percent of letters in under two minutes recovers around $130,000 of that. You can run the numbers for your own practice in our ROI Calculator. It takes three minutes, uses AUD figures, and requires no signup.
There is a second cost that shows up later. Practices where documentation dominates the end-of-day report higher staff dissatisfaction scores. Based on our work with Australian healthcare practices, once Claude is embedded and the workload shifts, the turnover picture improves. That implicit saving often lands between $80,000 and $100,000 per year in reduced recruitment and onboarding cost.

Build the privacy and audit layer first
The Privacy Act 1988, the Healthcare Identifiers Act 2010, and state-level health privacy legislation all govern how patient data can be handled in this workflow. A data handling error in this context does not just attract a fine. It can cost the practice its RACGP accreditation.
The deployment pattern that works here runs Claude inside the practice's existing cloud account, using AWS Bedrock or Google Vertex AI depending on what the practice management system already integrates with. No patient data flows to Anthropic's hosted API. Prompts, logs, and outputs stay within the practice's cloud perimeter. The practice retains healthcare information custodianship throughout, and audit logs live in the practice's own infrastructure.
This is not optional architecture. The privacy and audit layer goes in first. The drafting workflow goes on top of it.
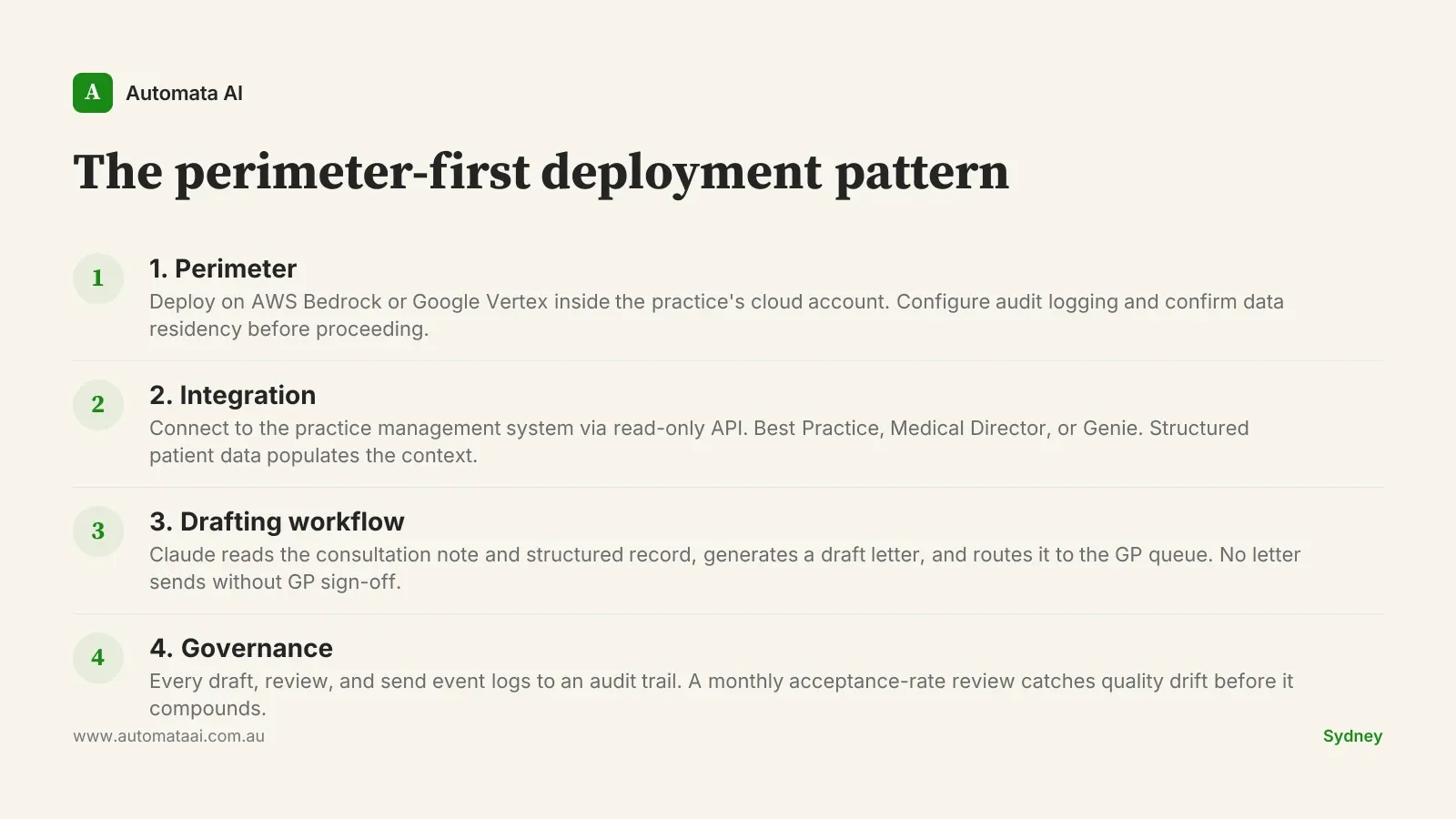
The perimeter-first deployment pattern
The pattern that works across Australian general practice has four phases. The order matters. Practices that skip phase one to get to the drafting workflow faster spend the next three months unpicking compliance issues.
Perimeter. Deploy Claude on AWS Bedrock or Google Vertex inside the practice's existing cloud account. Configure audit logging. Confirm data residency. Nothing proceeds until this is solid.
Integration. Connect to the practice management system via read-only API. Best Practice, Medical Director, or Genie, depending on the practice. Structured patient data, medications, and diagnostic history populate the prompt context.
Drafting workflow. Claude reads the consultation note and structured record, generates a draft letter, and routes it to the GP queue for review. No letter sends without GP sign-off.
Governance. Every draft, review, and send event logs to the audit trail. A monthly acceptance-rate review catches quality drift before it compounds.
What moves to Claude, what stays with the GP
The split is consistent across regulated Australian sectors. Drafting, summarising, and cross-referencing move to Claude. The referral letter gets drafted from the consultation note. The allied health summary pulls from the existing medication list and diagnostic history. The WorkCover certificate is pre-populated from structured data already in the record.
The GP reviews before send. Every time. That is not a workaround. It is the governance requirement and the correct clinical model. Claude is not making a clinical decision; it is doing the documentation work so the GP can make a faster, better-informed one. The distinction matters, especially when a letter touches a specialist or a regulator.
Decisions, attestations, and correspondence with oversight bodies stay with the qualified human. The letters arrive at the GP's desk drafted, not blank.
When this approach doesn't apply
Not every practice is ready, and not every letter type is a good early candidate.
The practice management system doesn't have a clean API. Some installations of Best Practice and Medical Director have integration limitations that make read-only data access messy. If data extraction requires workarounds, fix the integration layer first.
Letter volume is too low. If the practice generates fewer than 30 letters per week, the payback period stretches past 18 months. The effort is real; the return at that scale is not.
There is no one to own the governance layer. Claude GP letter drafting requires someone inside the practice who will own the audit trail, review the acceptance rate monthly, and flag when draft quality slips. Without that person, the workflow degrades silently.
If any of these apply, fix the prerequisite rather than pushing ahead. Practices that ship too early see adoption rates below 30 percent and typically abandon the workflow within the quarter.
The rollout discipline
Pilot with three GPs at one practice over six weeks. Measure two things: draft acceptance rate and average edit time per letter. If acceptance is above 80 percent and edit time is under two minutes per letter, promote to the full practice. If not, look for the pattern in what is being rejected. It is usually a specific letter type, or a data quality issue in the system. Fix it before expanding.
Practices that skip the pilot and roll to all GPs simultaneously see adoption rates below 30 percent. Practices that run the six-week pilot properly and promote on the basis of data hit adoption above 70 percent by month four. An AI Readiness Assessment before the pilot helps identify integration and governance prerequisites, so the six weeks are spent on drafting quality, not infrastructure.
The GP at 7:15pm writing referrals is not the unavoidable cost of running a practice. It is the avoidable cost of running a practice without the right workflow. Build the privacy layer first. Pick three letter types that cover the highest volume. Run the pilot. The drafting time comes back within weeks. The clinical energy that comes with it takes a little longer to notice, but it does come back.